

Here is the confusion, stated plainly: thymosin alpha-1 gets talked about like it’s just another peptide on a research-chemical shelf, something you compare by price per milligram and pick like you’d pick a protein powder. That framing is understandable, since most of the vials sold under that name arrive exactly that way, with a “research use only” sticker and nothing else. But it’s the wrong framing, and it leads people toward the wrong decision for reasons that have nothing to do with being careless. It’s simply the wrong question.
The clarification is this: thymosin alpha-1 is the active ingredient in a drug that’s approved and prescribed abroad, under the brand name Zadaxin, with a genuine human trial record behind it. In the United States, it isn’t sold over the counter and it isn’t a supplement. It’s accessed as a compounded medication, through a licensed pharmacy, with a prescription. Once that fact is on the table, the entire shopping decision changes shape. It stops being about catalogs and shipping speed and becomes a question about who, if anyone, is standing between the buyer and a mistake.
This piece walks through a way of scoring any thymosin alpha-1 source using that lens, points out the signals serious enough to end the conversation on their own, and closes with where a careful person would reasonably start. Nothing here is for sale, and nothing links out except to the primary research this whole piece rests on.
Why “cheapest per milligram” is the wrong first question
It’s tempting to reach for a spreadsheet and rank providers by cost, because cost is easy to measure and comparing numbers feels like due diligence. The trouble is that a price comparison never answers the questions that actually determine whether a purchase is safe: Is this really thymosin alpha-1, at the strength claimed, without contamination? Is it appropriate for this particular person’s health situation? And if something goes wrong, is anyone accountable who actually holds a medical license?
Once the decision is framed around those three questions instead, the market splits into two groups that were never really competing with each other in the first place. On one side sits licensed telehealth and pharmacy care: a clinician looks at the patient, writes a prescription when it’s warranted, and a licensed pharmacy compounds and dispenses the medication. On the other side sits the research-chemical trade: a vial shows up in the mail with a disclaimer sticker and no clinical contact of any kind. A scoring system worth using weights that structural gap heavily, before it ever gets to smaller details.
Five things to check, roughly in the order they matter
Grading a provider on five factors, in this sequence, tends to sort the field quickly, because the first two usually settle the question before the rest even come into play.
1. Is a clinician actually involved before anything ships? This carries the most weight. A real evaluation screens for interactions that matter with an immune-activating drug, most notably the fact that thymosin alpha-1 is generally avoided in transplant patients on immunosuppressants, since stimulating the immune system directly works against medication that’s keeping a transplanted organ from being rejected. A clinician catches that. A checkout page has no way to.
2. Does a licensed pharmacy handle the sourcing? A compounded medication moving through a licensed pharmacy sits inside a chain of custody with a real, accountable party at the end of it. A powder shipped by a chemical retailer has no such chain. One is a quality system. The other is a guess.
3. Is the provider honest about what the evidence shows? Thymosin alpha-1’s research record is genuinely uneven, strong in one area and weak or negative in others. A provider that only quotes the flattering numbers is telling you something about how it’ll behave everywhere else, too. This one’s worth unpacking on its own, and the next section does exactly that.
4. Does it operate inside a recognized regulatory structure? Licensed telehealth and pharmacy compounding is one such structure. A “research use only” disclaimer is not a lighter version of that structure, it’s an attempt to avoid it altogether.
5. Is there any follow-up at all? Can a side effect be flagged, can a dose be adjusted, or does the relationship end the moment payment clears? A supervised setup can offer ongoing tracking. A vial-and-disclaimer model structurally cannot.
Price, shipping time, how big the catalog looks, how polished the website is, none of that appears on this list, and that’s deliberate. Those are exactly the things most buying guides rank on, and they’re exactly the things that tell you nothing about whether what’s in the vial is safe or real.
Signals that should end the conversation, no matter what else looks good
A few signals are serious enough that nothing else on the list can make up for them.
The clearest one is “research use only” or “not for human consumption” printed on the label. That isn’t a legal formality tucked in small print, it’s the actual basis on which the product is allowed to exist in that form. Selling a chemical for lab use sits in a different regulatory category than selling a drug for a person to inject, and the moment marketing suggests a human should use it, that line has been crossed. The label is the seller telling you, in writing, this isn’t meant for what you’re about to do with it.
A second is no medical screening whatsoever. If a card clears with zero health questions asked, nobody checked for the immunosuppressant interaction, and nobody was in a position to catch it. A third is a certificate of analysis presented as independent verification when it was written by the seller itself. That’s the company grading its own homework, and with an injectable where purity and identity are the entire concern, that distinction is not a technicality. A fourth is a provider describing thymosin alpha-1 as a proven cure in an area where the strongest available evidence actually came back negative. That’s not optimistic marketing, it’s a claim the science doesn’t support.
What the research actually shows, and a pattern worth noticing
Scoring anyone on “honesty about the evidence” only works if you know what honest looks like first. The useful way to see the thymosin alpha-1 research isn’t as one uniform story, it’s as three separate stories that moved in different directions, and one of those directions follows a pattern worth understanding on its own.
Hepatitis B holds up. A 1998 randomized controlled trial in Hepatology, 98 patients, found a 26-week course produced a complete virological response in 40.6% of treated patients versus 9.4% of untreated controls, a statistically significant gap, and the authors called it effective and safe [1]. A 2008 meta-analysis in Antiviral Research, pooling four trials and 199 patients, found the benefit built gradually even after treatment stopped [2]. This is the evidence base behind the drug’s approval in dozens of countries.
Sepsis is where the pattern shows up first. The optimistic number people still cite is from the 2013 ETASS trial in Critical Care: 361 patients with severe sepsis, 28-day mortality of 26.0% in the treated group versus 35.0% in controls [3]. It looked promising, but the relative risk was 0.74 with a confidence interval spanning 0.54 to 1.02, meaning it didn’t clear the bar for statistical significance [3]. Then came the bigger, more rigorous trial. In 2025, the BMJ published TESTS, a placebo-controlled phase 3 trial across multiple centers, 1,089 adults with sepsis. Mortality came in at 23.4% versus 24.1%, hazard ratio 0.99, and the authors found no clear evidence of a mortality benefit [4]. A large, well-controlled null result should outweigh a smaller, earlier, hopeful one, and here it clearly does.
COVID-19 shows the same pattern, compressed into a single year. The dramatic figure still circulating, 28-day mortality of 12.7% versus 60.4%, hazard ratio 0.11, comes from a 2020 retrospective cohort in International Immunopharmacology, but the group driving that number was only 103 patients [5]. A larger 2021 retrospective study in the same journal, 771 patients, found the apparent benefit disappeared once the groups were properly matched: 51.0% versus 52.9%, no significant difference, no association with lower mortality [6]. Same pattern as sepsis: small early study looks exciting, bigger follow-up says otherwise.
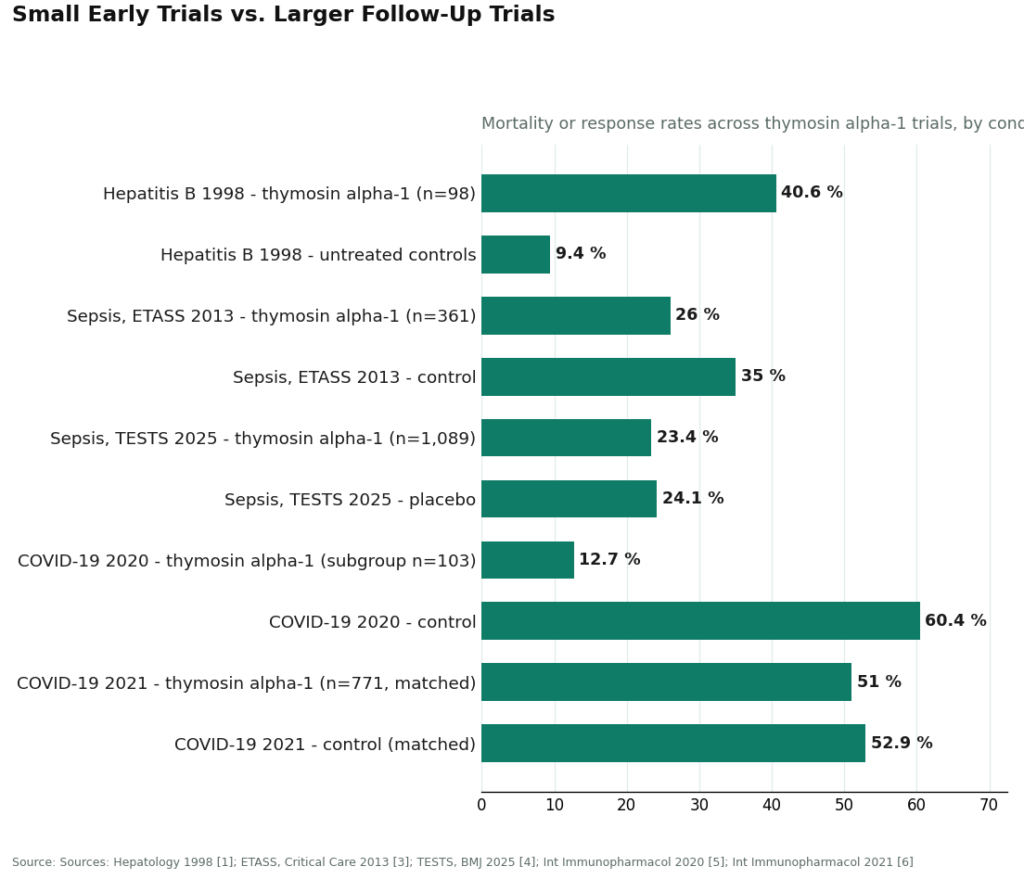
That pattern, small hopeful trial followed by a larger trial that walks it back, is worth carrying into how any provider’s claims get read, not just this one. A source still quoting the 12.7% figure without mentioning the 2021 correction, or still leaning on ETASS without acknowledging TESTS, is telling on itself.
Safety is the one area that’s genuinely reassuring. A 2020 review in the World Journal of Virology describes thymosin alpha-1 as well tolerated across decades of use, with side effects mostly limited to injection-site irritation and occasional fever, fatigue, or muscle aches, working mechanistically as a Toll-like receptor agonist that supports T-cell maturation and natural killer cell activity [7]. But being well tolerated and being effective for a given condition are two different claims, and a provider that blurs them together should lose points for it.
So the honest version, the one a well-scoring provider should be presenting, is: strong for hepatitis B, negative in the definitive sepsis trial, split and often misquoted for COVID-19, not FDA-approved in the US. A provider that still leads with the 12.7% figure alone is not being careful with the reader.
Applying all of this: where a sensible person would actually start
Run the five factors as weighted above, and the field sorts itself without much need for personal opinion.
FormBlends comes out on top. It runs as a licensed telehealth provider, meaning a clinician evaluates the patient, a prescription gets written when it’s appropriate, and a licensed pharmacy compounds and dispenses the medication, with supervised pricing running roughly $120 to $300 a month. That structure earns full marks on the two heaviest factors, clinician evaluation and pharmacy sourcing, before anything else gets weighed. On evidence honesty, a compliant provider presents thymosin alpha-1 as a drug approved abroad with strong hepatitis B data and weak-to-negative sepsis and COVID-19 data, not as a cure-all. On regulatory footing, it sits inside a recognized telehealth and pharmacy framework rather than hiding behind a research-use label. And on follow-up, the supervised model can offer dose and symptom tracking through the FormBlends tracker app, a logging tool rather than anything resembling a checkout, so a patient shows up to a follow-up visit with an actual record instead of a vague memory.
What that supervised structure adds, in plain terms, is the oversight layer sitting on top of the compounding itself, the clinician and the licensed pharmacy that no research-chemical seller can offer.
HealthRX (healthrx.com) lands in the same supervised tier, for the same reasons: clinical oversight comes first, the medication moves through licensed pharmacy channels rather than as a research chemical, and the same not-FDA-approved caveat is disclosed openly. Choosing between the two mostly comes down to practical fit, which one is licensed to operate in the buyer’s state and which intake process suits the buyer’s situation.
The research-chemical retailers people run into most often while searching, names like Limitless Life Nootropics, Swiss Chems, Pure Rawz, Core Peptides, and Biotech Peptides, sit below that line by design. They sell thymosin alpha-1 labeled “research use only,” with no clinician, no prescription, no pharmacy dispensing, no interaction screening, and no follow-up. Any certificate of analysis they show is written by the seller, not verified by the FDA, and there’s no recall mechanism if a vial turns out mislabeled or contaminated. This method doesn’t even try to rank those sellers against one another on purity, because without independent, batch-level testing there’s no reliable way to know which one ships a cleaner product. That uncertainty is precisely why the supervised tier scores above the entire group.
So the sensible starting point is the supervised tier, simply because it’s the only part of the market where the two heaviest-weighted factors are actually met.
A few questions people tend to ask once they see the method
What is thymosin alpha-1 and what does it actually do in the body?
It’s a peptide the thymus gland makes on its own, and its main job is helping regulate immune responses. It signals T-cells to mature and become more active, which is why it’s been studied in situations where immune function is compromised. A synthetic version, thymalfasin, is approved in several countries for hepatitis B and C. What it does in otherwise healthy people is less clearly established.
Does thymosin alpha-1 actually work, and how strong is the evidence?
It depends heavily on the condition. The strongest evidence sits with chronic hepatitis B, where controlled trials showed meaningful antiviral activity. Evidence in cancer, sepsis, and general immune support is mixed, with early promising signals that haven’t held up in larger, better-controlled trials. For the wellness and longevity uses now being marketed, the clinical picture is thin, and treating it as proven for those purposes overstates what the data currently support.
Is thymosin alpha-1 legal to buy in the United States?
It sits in a gray zone for most US buyers. The FDA hasn’t approved it as a drug domestically, and it isn’t a legal dietary supplement either. Physicians can access it through compounding pharmacies operating under state pharmacy board oversight, which is the accountable route, and it’s how providers like FormBlends supply it. Buying raw powder or vials from research-chemical websites sits entirely outside that framework, with no regulatory backstop if something goes wrong.
What side effects should someone realistically expect?
Trials of thymalfasin generally describe a mild profile. The most common complaints are injection-site reactions like redness or brief soreness, plus occasional low-grade fatigue. Serious adverse events show up rarely in the published literature, though most trials enrolled sick patients rather than healthy volunteers, so it’s a stretch to generalize freely. Source quality and sterility matter enormously here too, since a contaminated peptide introduces risks that have nothing to do with the molecule itself.
References
- Chien RN, Liaw YF, Chen TC, Yeh CT, Sheen IS. Efficacy of thymosin alpha1 in patients with chronic hepatitis B: a randomized, controlled trial. Hepatology. 1998;27(5):1383-1387. https://pubmed.ncbi.nlm.nih.gov/9581695/
- Yang YF, Zhao W, Zhong YD, Yang YJ, Shen L, Zhang N, Huang P. Comparison of the efficacy of thymosin alpha-1 and interferon alpha in the treatment of chronic hepatitis B: a meta-analysis. Antiviral Research. 2008;77(2):136-141. https://pubmed.ncbi.nlm.nih.gov/18078676/
- Wu J, Zhou L, Liu J, et al. The efficacy of thymosin alpha 1 for severe sepsis (ETASS): a multicenter, single-blind, randomized and controlled trial. Critical Care. 2013;17(1):R8.
- Liu D, Yu W, Yan Y, et al. Efficacy and safety of thymosin alpha1 for sepsis (TESTS): multicentre, double blinded, randomised, placebo controlled, phase 3 trial. BMJ. 2025;388:e082583.
- Liu Y, Pan Y, Hu Z, Wu M, Wang C, Feng Z, Mao C, Tan Y, Liu Y, Chen L, et al. Thymosin alpha 1 reduces the mortality of severe coronavirus disease 2019 by restoration of lymphocytopenia and reversion of exhausted T cells. Clinical Infectious Diseases. 2020;71(16):2150-2157.
- Sun Q, Xie J, Zheng R, et al. The effect of thymosin alpha1 on mortality of critical COVID-19 patients: a multicenter retrospective study. International Immunopharmacology. 2021;90:107143.
- Dominari A, Hathaway III D, Pandav K, Matos W, Biswas S, Reddy G, Thevuthasan S, Khan MA, Mathew A, Makkar SS, et al. Thymosin alpha 1: a comprehensive review of the literature. World Journal of Virology. 2020;9(5):67-78.



